Closing the perception vs. reality gap in oncology care: Why accurate near real-time clinical data is vital
Key Takeaways
- Physician surveys suggest high rates of biomarker testing, but real-world data reveals a significant gap, with testing rates being materially lower than perceived.
- Relying on incomplete data creates strategic risks for life sciences organizations, leading to flawed forecasting and commercial strategies built around the wrong bottlenecks.
- Next Intelligence integrates near real-time multimodal data to provide a more accurate view of the patient journey, enabling clients to identify specific breakdowns in care and develop targeted interventions.
Background
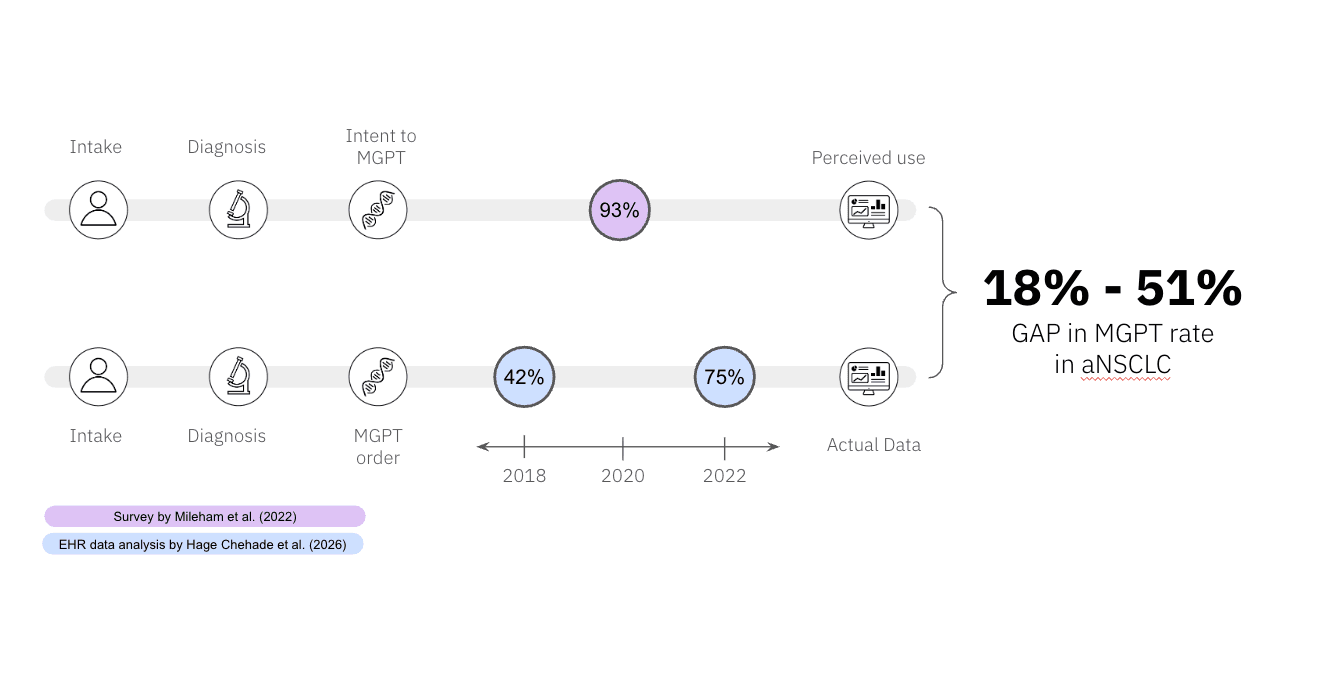
Precision oncology depends on timely, clinically meaningful biomarker testing, but our understanding of how often that actually happens is only as good as the data used to measure it. Different data sources can tell very different stories. Physician surveys may suggest high adherence to testing recommendations: for example, in a survey of U.S. oncologists published in Cancer Medicine in 2022, 93% of respondents reported ordering multi panel biomarker biomarkers for NSCLC patients.1 However, surveys capture reported practice, not the full clinical reality. They often fail to show:
- Whether testing was completed
- Whether results were returned in time to guide treatment
- Whether the assay itself was sufficiently comprehensive
Real-world clinical data often paint a more sobering picture.2,3 In a large national EHR-derived study published by JAMA Network in 2026, more than 30% of patients with advanced or metastatic solid tumors still did not undergo next-generation sequencing, and delays in testing were more common among patients with lower socioeconomic status.2 Even in advanced NSCLC—often viewed as a mature precision oncology setting—documented testing may overstate clinical readiness: differences in gene coverage, RNA fusion detection, assay sensitivity, and reporting can create what has been described as an "illusion of comprehensive testing."4
The illusion of a solved problem
The perception that biomarker testing for advanced NSCLC is essentially saturated, often reinforced by high self-reported testing rates in surveys, may be inaccurate as these figures reflect intended or recalled practice rather than verified care delivery.1
The implication is clear: if stakeholders rely on self-report, incomplete claims capture, or simple binary measures of whether a test occurred, they risk building strategies on the wrong picture of care. As Voruganti and colleagues have argued, assays labeled or perceived as comprehensive may still differ meaningfully in gene coverage, RNA fusion detection, analytical sensitivity, and reporting quality.4
As a result, the appearance of high testing uptake can mask important gaps in whether testing was timely, complete, and clinically actionable.
Uncovering the real care gap
To understand the true state of biomarker testing, no single dataset is sufficient. Surveys, claims, EHRs, and molecular testing data each capture different parts of the patient journey and each have important limitations. Integrating them can improve the completeness of patient journey mapping and help reveal where gaps actually occur. That matters because breakdowns can happen at multiple points in the care pathway. A test may be:
- Intended but not ordered
- Ordered but not completed
- Completed but not comprehensive
- Resulted too late to influence treatment
A multimodal approach makes it possible to move beyond a simple measure of whether testing occurred and instead identify the operational, clinical, and structural barriers that keep patients from receiving timely, guideline-concordant care.
Earlier analyses performed using this approach in advanced NSCLC pointed to a persistent testing rate between 70-80% in advanced NSCLC, a markedly different picture from the >95% rates often cited in commercial discussions.5 Those findings are now increasingly aligned with the published literature. The existence of this disparity is further substantiated by a recent study conducted by investigators from the University of Utah and Case Western Reserve. Their findings revealed that next-generation sequencing (NGS) rates for advanced lung cancer hovered between 61% and 65% from 2018 to 2022, highlighting a substantial gap in care.2
Contrasting Data Sources Highlight Discrepancies in MGPT Testing in aNSCLC
From insight to intervention
For life sciences organizations, the illusion of a solved problem is not just a measurement issue—it is a strategic risk. If testing rates are assumed to be 90% or higher when the real-world rate is materially lower, the result is not just a data error. It can lead to overstated market assumptions, flawed forecasting, and commercial strategies built around the wrong bottleneck.2 Just as importantly, high-level testing metrics can obscure the real barriers to therapy adoption, whether those barriers stem from incomplete testing, delayed turnaround times, assay limitations, workflow friction, or inequities across patient populations.
This is where Next Intelligence offers a different lens. By integrating multimodal data to create a more complete view of the patient journey, it can help organizations move beyond broad assumptions and toward a more precise understanding of where the pathway is breaking down. That clarity can inform not only how market opportunity is assessed, but also where interventions are most likely to have impact—whether through provider education, workflow redesign, testing optimization, or collaborative efforts to improve guideline-concordant care. In that sense, the value is not simply in showing that the problem is larger than expected; it is in making the gap specific enough to act on.
Next Intelligence provides near real-time intelligence to connect longitudinal patient data with codified standards of care, so that missed or delayed steps can be surfaced while intervention is still possible. In this way, the mission is not simply to report that a gap exists, but to help make that gap visible early enough, and clearly enough, to support action. That creates the bridge from better data to better strategy—and ultimately, to more consistent delivery of precision oncology in routine care.
Conclusion
Closing the gap between perception and reality in oncology testing starts with measuring the problem the right way. That means seeing enough detail to understand what is really happening in patient care.
When different data sources are brought together in the right way, they can show where testing is breaking down, which patients are being missed, and what barriers are getting in the way. That clearer view is what Next Intelligence is designed to deliver—helping health systems and life sciences partners move from assumption to action and build strategies that can meaningfully close gaps in precision oncology care.
References
- Mileham KF, Schenkel C, Bruinooge SS, et al. Defining comprehensive biomarker-related testing and treatment practices for advanced non-small-cell lung cancer: Results of a survey of U.S. oncologists. Cancer Medicine. 2022;11(2):530-538. doi:10.1002/cam4.4459
- Kehl KL. Biomarker Testing in Advanced Cancer. JAMA Network Open. 2025;8(7):e2519972. doi:10.1001/jamanetworkopen.2025.19972
- Hage Chehade C, Ozay ZI, Jo Y, et al. Trends and Disparities in the Use of Next-Generation Sequencing in Patients With Cancer in the United States. JAMA Network Open. 2026;9(4):e265585. doi:10.1001/jamanetworkopen.2026.5585
- Voruganti T, Wang X, Marmarelis ME, et al. Illusion of Comprehensive Testing in Non–Small Cell Lung Cancer: Why Coverage, Sensitivity, and Reporting Matter. JCO Oncology Practice. 2026. doi:10.1200/OP-25-01350
- Case Study: Tempus Next Pathways unlocked critical insights into the aNSCLC patient journey with Bristol Myers Squibb (BMS).


