Constructing clinical timelines with line of therapy
Understanding a patient’s treatment history is fundamental to oncology research, which requires the concept of line of therapy (LoT). Clinical records from real-world practice are inconsistent in the capture of LoT, both in coverage and definition. Tempus addresses this challenge by applying consistent rules for assigning LoTs based on clinical documentation.
The critical role of line of therapy
Lines of therapy are a key anchor for benchmarking therapy performance and informing R&D strategy, including when comparing patient outcomes and drug effectiveness over time and across cohorts. They enable clinical insights into treatment patterns, time-to-progression, and survival, and support research and regulatory use cases where treatment sequencing is critical.
Establishing scale across solid and heme indications
A line of therapy is a planned regimen consisting of one or more antineoplastic medications, in combination or in sequence, with the potential addition of radiotherapy. Each LoT is assigned a serial, chronologically ordered number. This framework, along with a number of other rules, forms the foundation for Tempus’s general pan-cancer guidelines. While general principles provide a standardized baseline, applying a single, uniform set of rules across all cancer types risks either over-counting or under-counting LoTs in some indications. To prevent this and accurately capture patient treatment courses, we systematically refine our pan-cancer general guidelines to accommodate the unique clinical practices of specific indications.
Tempus has developed standardized, expert-vetted guidelines to assign LoTs for an extensive range of cancer types. Among solid tumors, these include Breast, Lung (NSCLC and SCLC), Colorectal, Pancreatic, Ovarian, Prostate, Melanoma, Bladder, Gastric, Esophageal/EGJ, and Head and Neck cancers. Among hematologic malignancies, these include Plasma Cell Neoplasms, Chronic Lymphocytic Leukemia (CLL/SLL), and various lymphomas, including Large B-Cell and Follicular Lymphoma.
Our rules are tailored for each indication based on expert guidance. The process begins with our clinical team reviewing NCCN guidelines and other literature for a given indication to ensure that the rules are grounded in how LoTs are defined in real-world clinical practice and research. The rules are then reviewed by an oncologist serving as a subject matter expert for that indication. An example indication-specific rule is that for ovarian cancer, clinical consensus dictates that LoT numbering begins at the start of treatment, while for other solid tumors, LoT numbering begins in the metastatic or unresectable setting.
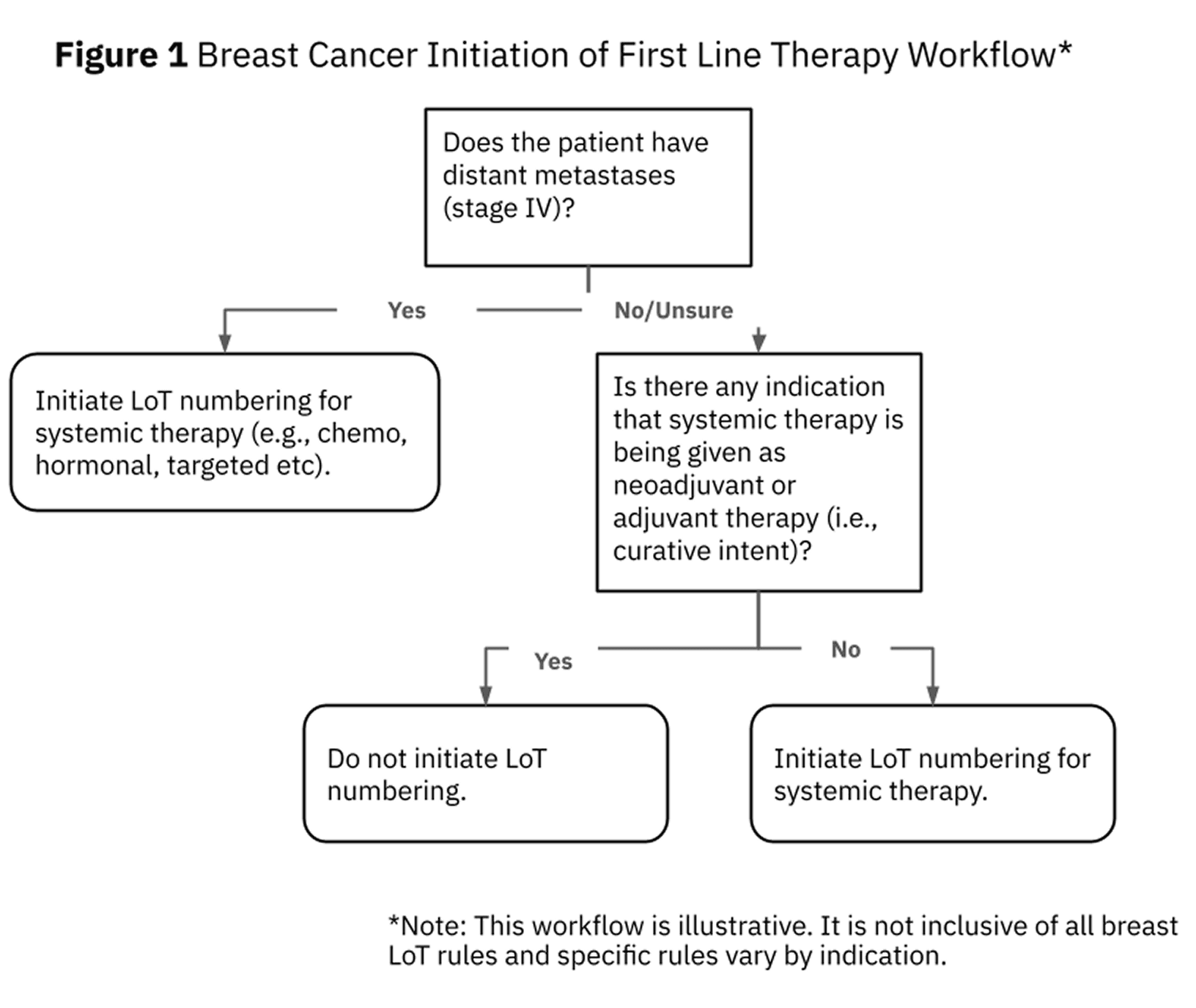
An example of the reasoning behind LoT assignment is shown in Figure 1. Breast cancer LoT numbering begins when the patient has disease that is not amenable to definitive surgery, in other words, in the metastatic or unresectable setting.
For each patient, once LoT numbering is initiated, rules dictate when treatment is considered a new line, most commonly when the regimen is changed due to progression. Our guidelines cover an extensive number of scenarios. For example, maintenance therapy is included in the same line, while a regimen change based on new biomarker information initiates a new line.
Building a foundation for high-impact research
A transparent, rules-based LoT framework does more than organize records; it facilitates a longitudinal view of the evolution of disease.
As a critical element within our clinical data, LoTs also provide clinical context when combined with our molecular data. This combination enables researchers to evaluate genomic alterations within the framework of a patient’s treatment history, including the timing of sample collection relative to each LoT. By anchoring molecular insights to clear and standardized clinical events, researchers can interrogate mechanisms of resistance and the nuances of drug durability with better precision.
Whether identifying patient populations based on prior treatment failures or stratifying cohorts by biomarker expression and regimen within a given line, this standardized foundation enables researchers to proceed directly to analysis with confidence. As Tempus’ data library continues to mature, we remain committed to providing these high-quality clinical concepts, ensuring that as our data volume increases, so does the depth and reliability of your research.


