-
PROVIDERS
REGISTER NOW
Upcoming Webinar:
MRD data insights across the cancer care continuum -
LIFE SCIENCES
REGISTER NOW
From insight to impact: Leveraging the AI-enabled Next platform with BMS to advance equitable access in precision oncology
-
PATIENTS
It's About Time
View the Tempus vision.
- RESOURCES
-
ABOUT US
View Job Postings
We’re looking for people who can change the world.
- INVESTORS
02/17/2026
Signal-to-Noise Ratio in 4D Flow CMR: Sequence Determinants and Impact on Kinetic Energy, Energy Loss, and Vorticity – Insights from the TREK Study
Journal of Cardiovascular Magnetic Resonance
PRESENTATION
Authors
Marc Lee, Ryan O'Hara, Jared Klein, Richard Friesen, Matthew Dove, Anudeep Dodeja, Hieu Ta, Jonathan Kochav, Adam Christopher, Rajesh Krishnamurthy, Elias Balaras, Francesco Capuano, Brett Meyers, Yue-Hin Loke
Background: Advanced 4D flow cardiac magnetic resonance (CMR) biomarkers such as kinetic energy (KE), energy loss (EL), and vorticity are increasingly applied to characterize congenital heart disease such as repaired Tetralogy of Fallot (rTOF). However, use in pediatric populations often involves variation in acquisition parameters and image quality, which may impact hemodynamic measurements and confound physiologic interpretation. Understanding both the determinants of signal-to-noise ratio (SNR) and its independent impact on derived flow metrics is critical for harmonization and multicenter adoption.
Methods: We analyzed 276 complete 4D flow CMR datasets across six institutions from the multicenter Tetralogy of Fallot 4D flow Registry of Energetics and Kinetics (TREK) study (rTOF patients and controls, median age 19 years, 46% female). Imaging was performed on 1.5T and 3T Siemens/GE scanners with varying voxel sizes, flip angles, temporal resolutions, and contrast protocols. Sequence metadata were extracted. SNR was measured via ROI analysis on Pixel (Tempus), defined as the ratio of peak aortic signal intensity to standard deviation of air signal intensity. 4D flow biomarker extraction was performed using ITFlow (CardioFlow Design, Tokyo, Japan), yielding mean systolic KE (mJ/mL), mean systolic EL (mW/mL), and peak systolic vorticity (1/s). Multivariable models evaluated (1) sequence determinants of SNR, and (2) independent associations of SNR with flow biomarkers after adjustment for case type and clinical covariates (BSA, rTOF vs control, ventricular size/function).
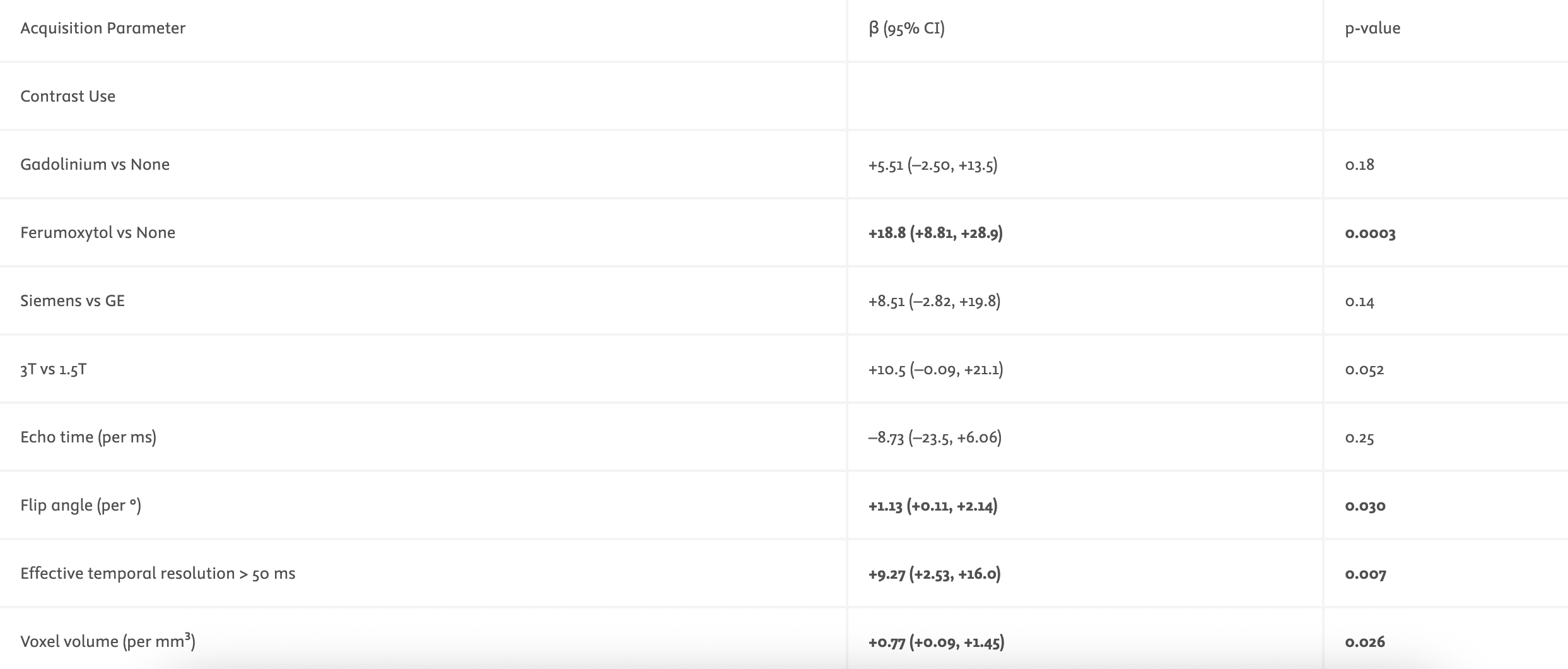
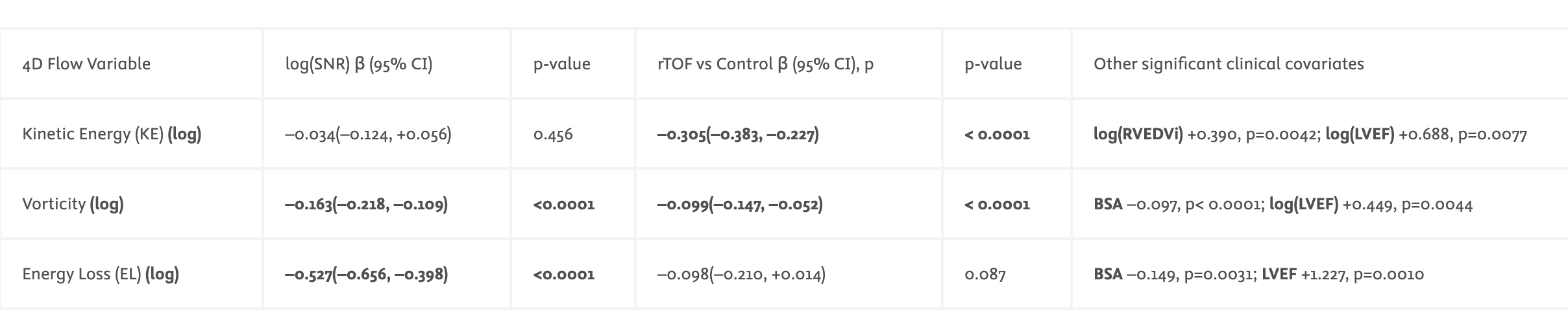
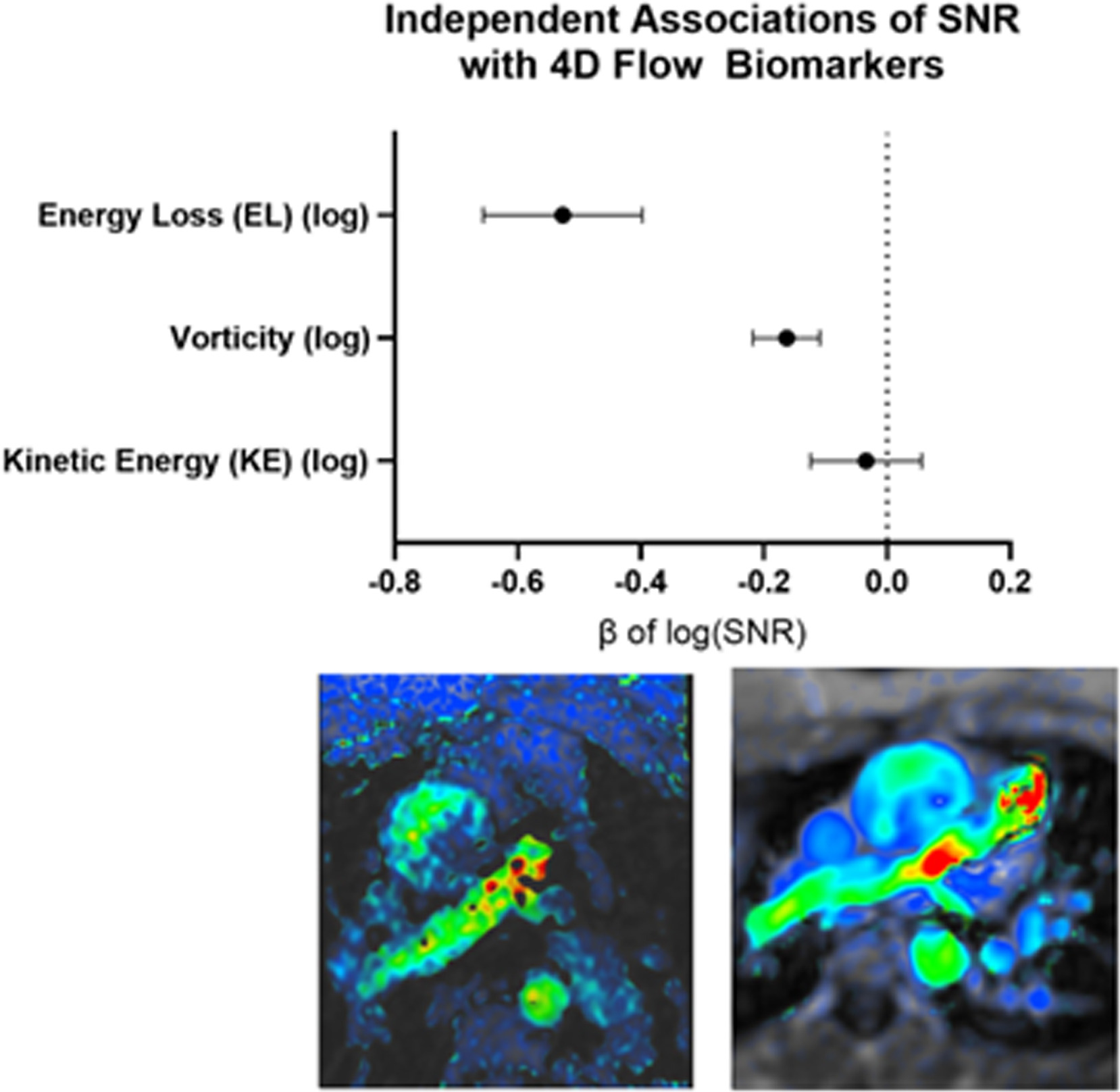
Results: SNR was strongly influenced by acquisition parameters (Table 1), with significant independent contributions from voxel volume (p=0.026), flip angle (p=0.030), temporal resolution >50 ms (p=0.007), and the use of ferumoxytol agent (p< 0.001). Field strength showed a trend toward higher SNR at 3T vs 1.5T (p=0.052), while vendor (Siemens vs. GE) and echo time were not significant. For the 4D flow biomarkers (Table 2) after adjusting for clinical variables, SNR was independently associated with EL (β=–0.53, p< 0.0001) and vorticity (β=–0.16, p< 0.0001), but not KE (β=–0.03, p=0.46). Lower SNR inflated EL and vorticity values (Figure 1). KE in the aorta was unaffected by SNR, and was significantly lower in rTOF compared with controls (p< 0.0001), with further contributions from RVEDVi and LVEF.
Conclusion: SNR is determined by acquisition parameters, and in turn selectively influences downstream 4D flow biomarkers. EL and vorticity appear to be highly SNR-sensitive, whereas KE remains physiologically robust, demonstrating lower KE in rTOF patients which may have prognostic significance. These findings underscore the need to account for image quality in multicenter 4D flow studies and support harmonization strategies to ensure accurate interpretation of advanced flow metrics. Future work will assess cross-vendor reproducibility to enable reliable clinical translation.
-
 04/21/2026
04/21/2026Tempus Next Pathways unlocked critical insights into the aNSCLC patient journey with Bristol Myers Squibb (BMS)
Discover how BMS collaborated with Tempus to deploy the Next Pathways program across 13 community-based health systems to address care gaps for patients with advanced non-small cell lung cancer (aNSCLC).
Read more -
 04/02/2026
04/02/2026Unlocking foundation models: Our experience from proof of concept to deployment at scale
An executive discussion on leveraging multi-modal foundation models to accelerate your drug development journey
Watch replay -
 04/03/2026
04/03/2026Utilizing real-world external controls for regulatory decision-making
A biotech company needed to contextualize its Phase 1b/2a trial for mNSCLC patients with a specific mutation. Learn how Tempus constructed a real-world external control arm to provide a benchmark for their regulatory submission.
Read more