-
PROVIDERS
New MRD Medicare Coverage for Select Indications*
*When coverage criteria are met. Additional criteria and exceptions for coverage may apply.
-
LIFE SCIENCES
Register now
UPCOMING WEBINAR
Unlocking Foundation Models: Our experience from proof of concept to deploying at scale -
PATIENTS
It's About Time
View the Tempus vision.
- RESOURCES
-
ABOUT US
View Job Postings
We’re looking for people who can change the world.
- INVESTORS
11/04/2025
Ultrahigh Tumor Mutational Burden (TMB) Is Associated With Improved Survival Outcomes in Patients (Pts) Treated With Immune Checkpoint Inhibitors (ICIs)
SITC 2025
PRESENTATION
Authors
Douglas B Johnson, Binyam Yilma, Stamatini Fragkogianni, Metamia Ciampricotti, Tina O’Grady, Ben Ho Park, Justin M Balko
Abstract
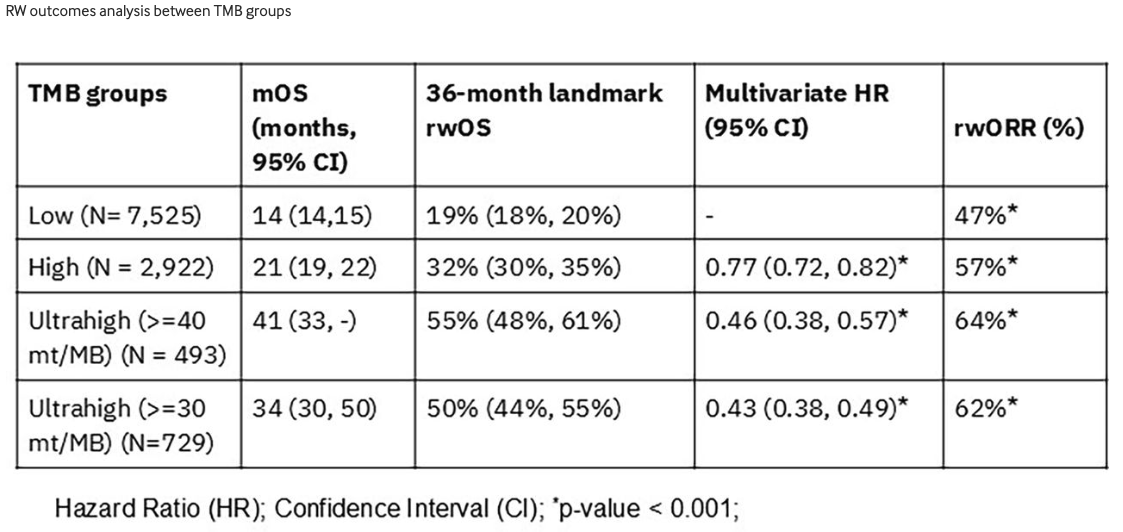
Background – TMB is associated with response to ICI therapy (tx). A pan-tumor cutoff of 10 mutations (mt)/MB gained FDA approval of pembrolizumab although optimal cutoffs are not clearly defined. Here, we assessed the genomic landscape and clinical outcomes and in pts with higher cutoffs of 30 and 40 mt/MB (‘ultrahigh TMB’).
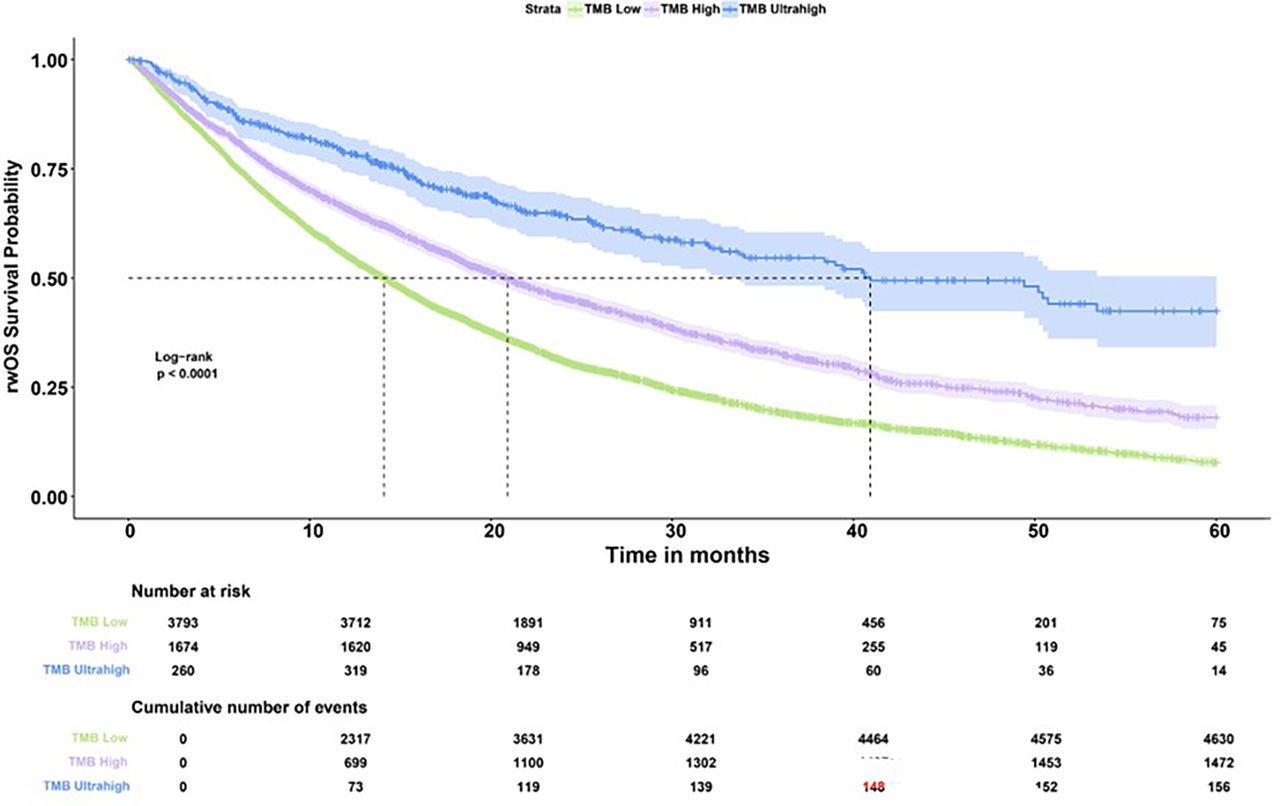
Methods – We used Tempus Lens (Tempus AI, Inc., Chicago, IL) to identify patients with melanoma, non-melanoma skin cancer (NMSC), lung, uterine, and gastrointestinal (GI) cancers who had Tempus xT (DNA-seq) testing and immune checkpoint inhibitor (ICI) treatment data available in the Tempus multi-modal database (N=17,449). Patient samples obtained within one year before or 15 days after starting ICI therapy (N=11,581) were grouped by TMB into low (<10) (N=7,953), high (>=10) (N=3,082), and ultrahigh (>=40) (N=546). Immune cell proportions (%) were estimated from RNA using quanTIseq. Real-world (rw) objective response rates (rwORR) were assessed at 365-days after ICI tx start, and compared using Pearson’s Chi-Squared test. RW overall survival (rwOS) was defined as time from ICI start to death, lost to follow-up. Median rwOS was estimated using Kaplan-Meier (KM) and hazard ratios (HR) using Cox proportional hazard models.
Results – Demographic characteristics including age and sex were similar between groups. Among the ultrahigh group, 266 (49%) had GI cancer, 82 (15%) had lung cancer, 117 (21%) had melanoma, 38 (7%) had NMSC, and 43 (8%) had uterine cancer. rwORR was significantly higher in the ultrahigh group compared to the high and low groups (p<0.001) (table 1). This trend was more pronounced in melanoma, lung, and GI cancers compared with NMSC and uterine cancer. rwOS was significantly improved in pts in the ultrahigh and high TMB groups compared to the low group (HR 0.38, 0.69, p<0.001) (figure 1). Results remained significant when adjusting for cancer type, MSI status, stage, age, and sex (table 1). Similar results were seen using a 30 mt/MB cutoff. Immune cell infiltration was higher in the ultrahigh TMB group for CD8, regulatory T-cells, M1 macrophages, and neutrophils, and lower for B cells and M2 macrophages (p<0.001). Most gene mutations were more common in ultrahigh TMB samples except TP53, KRAS, and MTAP.
Conclusions – Ultrahigh TMB (>=40 mt/MB) comprises a novel marker for ICI response and is characterized by higher degree of T cell and myeloid cell markers.