-
PROVIDERS
New MRD Medicare Coverage for Select Indications*
*When coverage criteria are met. Additional criteria and exceptions for coverage may apply.
-
LIFE SCIENCES
Register now
UPCOMING WEBINAR
Unlocking Foundation Models: Our experience from proof of concept to deploying at scale -
PATIENTS
It's About Time
View the Tempus vision.
- RESOURCES
-
ABOUT US
View Job Postings
We’re looking for people who can change the world.
- INVESTORS
10/02/2025
SERENA-6 Q&A: An author’s insights on clinical integration and future directions
This Q&A features Dr. Cynthia Ma, breast medical oncologist at Washington University and SERENA-6 co-author, in conversation with Dr. Gary Grad, Senior Medical Oncologist at Tempus, on the groundbreaking findings from the SERENA-6 trial and the impact on patient management.
Speakers
Cynthia X. Ma, MD, PhD
Washington University School of Medicine

Gary Grad, MD
Senior Medical Oncologist, Tempus

Washington University School of Medicine
Gary Grad, MD
Senior Medical Oncologist, Tempus
Introduction
In the evolving era of ctDNA testing, the insights from the SERENA-6 trial highlight the value of sensitive detection of emerging ESR1 mutations – an area where Tempus xF+ provides actionable solutions to support earlier intervention and more personalized management of ER-positive, HER2-negative breast cancer. Clinical background & study rationale
Dr. Gary Grad: Can you start by telling us about your background and your role in the SERENA-6 study? |
| Dr. Cynthia Ma: I’m a breast medical oncologist, physician-scientist, and a professor of medicine at Washington University in St. Louis. My interests include biomarker-directed clinical trials, particularly those focused on mechanisms of endocrine resistance and resistance to CDK4/6 inhibitors. I served on the SERENA-6 steering committee, contributed to study design and execution and was the clinical investigator at our site. |
Dr. Gary Grad: Fantastic. ESR1 has been a known target for a long time, emerging as an acquired resistance mechanism. Can you discuss the hypothesis the steering committee had when designing SERENA-6? |
| Dr. Cynthia Ma: We know that metastatic ER-positive, HER2-negative breast cancer remains incurable at this time. CDK4/6 inhibitors have significantly improved outcomes, but most patients eventually progress on first-line therapy. Among those receiving an aromatase inhibitor plus a CDK4/6 inhibitor, approximately 40% develop an ESR1 mutation, which is a key driver of acquired endocrine resistance, particularly to aromatase inhibitors. Historically, treatment changes are made only at radiographic progression, by which point tumor burden is often higher and therapeutic options more limited. SERENA-6 was designed to intervene before radiographic progression, at the point of molecular detection of ESR1 mutation, to test whether early switching could prolong progression-free survival on CDK4/6 inhibitors and help preserve quality of life. |
Study design & endpoints
Dr. Gary Grad: Could you briefly describe the design of the SERENA-6 study, including its primary and secondary endpoints, and why this specific design was chosen to address the clinical question? Beyond the clinical endpoints, what were the key takeaways regarding patient-reported outcomes or quality of life in the SERENA-6 study? |
| Dr. Cynthia Ma: Patients with ESR1 mutations detected during screening, but without radiographic progression, were randomized to either continue their AI plus CDK4/6 inhibitor or switch the AI to camizestrant while maintaining the same CDK4/6 inhibitor. The trial was a double-blind, placebo-controlled design. The primary endpoint was progression-free survival: early switching to camizestrant upon ESR1 mutation detection, before radiographic progression, achieved a median PFS of 16. 2 months compared to about 9 months for the control group, indicating a significant improvement. In addition, patients completed quality-of-life questionnaires. Those in the early-switching arm taking camizestrant, showed a markedly delayed deterioration in global health status—21 months versus just over 6 months in the control arm, which is a very significant finding. Camizestrant was well tolerated, with side effects generally related to CDK4/6 inhibitors, such as grade 3 neutropenia. There were low-grade visual disturbances like photopsia related to camizestrant, which were manageable and non-structural. |
Quality of life & clinical implications
Dr. Gary Grad: Do you think the quality-of-life benefit was due to delayed disease progression, staying on endocrine therapy longer as opposed to getting on cytotoxic or ADC treatments, or something else? |
| Dr. Cynthia Ma: I think the quality-of-life benefit was primarily due to preventing symptomatic progression. Measures like pain, which often serve as early indicators of disease progression, and other functional and symptom scores showed earlier time to deterioration in the control group, around 6 months. In contrast, patients on camizestrant experienced a much longer delay in these declines, consistent with the extended disease control observed in the trial. |
Dr. Gary Grad: So, even if the trial doesn’t show an overall survival advantage, then PFS, delaying time to next treatment, and preserving quality of life are clinically meaningful endpoints. This could shift our paradigm from relying solely on OS to recognizing impactful outcomes beyond survival. |
| Dr. Cynthia Ma: Yes, I agree. |
Dr. Gary Grad: Are there specific patient profiles more or less suitable for this monitoring and therapy-switch approach? Or do you think it applies to all HR+/HER2- patients? |
| Dr. Cynthia Ma: SERENA-6 enrolled patients who had received at least 6 months of first-line therapy with an AI plus a CDK4/6 inhibitor without radiographic progression. This design was selected for a more endocrine-sensitive population with ER-driven biology. Rapid progressors may not benefit from this approach. |
ctDNA insights into ESR1 emergence
Dr Gary Grad: Regarding ESR1 detection dynamics, what ctDNA monitoring insights can we draw for real-world application, assuming camizestrant gains approval? |
| Dr. Cynthia Ma: Currently, ctDNA testing is typically done at baseline and at radiographic progression to identify actionable mutations. SERENA-6 introduces a paradigm shift by demonstrating that early intervention upon detection of ESR1 mutations, prior to radiographic progression, can potentially improve clinical outcomes. While the trial didn’t explicitly evaluate optimum ESR1 testing frequency, the approach taken in SERENA-6 of monitoring ESR1 mutations every 2–3 months, aligned with office visits and imaging, offers a practical and clinically meaningful strategy. In addition to practical concerns, the implementation of this approach will also depend on insurance coverage and FDA-approval. |
Dr. Gary Grad: Were there any observable trends in ESR1 mutation emergence over time? |
| Dr. Cynthia Ma: Yes. Data from the PADA-1 trial showed that the highest incidence of ESR1 emergence occurred between 6 and 30 months of treatment, with lower rates before 6 months or after 30 months. These findings can help prioritize which patients might benefit the most from monitoring. |
Dr. Gary Grad: Regarding different ESR1 mutations, and patients with multiple mutations, did the study identify differences in response to camizestrant? What about co-mutations, like PIK3CA, or germline variants? |
| Dr. Cynthia Ma: Benefit was seen across all ESR1 mutation types, whether single or multiple. No definitive conclusion favors acting on one mutation over another. Analyses for co-mutations are still pending. |
Clinical applications & future directions
Dr. Gary Grad: SERENA-6 has received a lot of attention since its presentation at the 2025 ASCO® Annual Meeting. How are you discussing ctDNA monitoring and camizestrant with patients currently, given it’s not yet approved? |
| Dr. Cynthia Ma: I talk with patients about the data and the concept of molecular surveillance. In the absence of camizestrant approval, alternatives such as fulvestrant can be considered. There are also phase 1 safety data for options such as elacestrant in combination with CDK4/6 inhibitors, though insurance coverage may present a barrier. I discuss these treatment options, along with the logistics, potential burdens of surveillance, and consider early therapy switches on a case-by-case basis with each patient. |
Dr. Gary Grad: As we think about this paradigm shift—identifying an acquired resistance mechanism and targeting it—there’s the broader concept of monitoring molecular progression before clinical or radiographic progression, which brings us into the era of MRD testing. Do you foresee a time when ultra-sensitive MRD assays, detecting molecular progression at very low levels, might help guide earlier decisions about transitioning patients to the next line of treatment before radiographic progression? |
| Dr. Cynthia Ma: Yes, I believe SERENA-6 provides strong evidence that when an effective agent is available, targeting emerging resistance can improve patient outcomes. If our therapies can overcome these resistance mechanisms, MRD assays could potentially detect resistant clones earlier, allowing for timely intervention. This approach may represent the future of cancer treatment. Of course, prospective trials will be essential to validate this approach, but it holds promise for shaping future cancer therapy strategies. |
Dr. Gary Grad: We know not every patient develops ESR1 after progression on a CDK4/6 inhibitor, and some may instead have other actionable variants—like PIK3CA, germline BRCA, or even HER2-low or ultralow status. Do you see the potential to apply a similar paradigm of switching therapy earlier based on molecular progression—whether detected by MRD or other biomarkers—even in patients without ESR1? In other words, could this approach be extrapolated to other actionable biomarkers where targeted therapies exist? |
| Dr. Cynthia Ma: Yes, I think that’s possible. When we talk about switching therapies, we always have to weigh not only efficacy but also quality of life. SERENA-6 highlighted that camizestrant was not only effective but also well tolerated. One concern with switching early is whether the next therapy will be tolerable. But as we see the development of more tolerable targeted agents, such as newer PIK3CA inhibitors and other targeted agents in the second-line setting, I do think applying this kind of paradigm more broadly could become a reality. |
Closing thoughts
Dr. Gary Grad: You’ve already mentioned some of the future studies that will come out of SERENA-6 in terms of refining cohorts such as co-mutations. What excites you most about the treatment landscape for ER-positive, HER2-negative breast cancer moving forward? |
| Dr. Cynthia Ma: The large number of novel selective estrogen receptor degraders, other exciting ER-targeting agents, combinations with CDK4/6 inhibitors, and mutation-selective PIK3CA inhibitors are all very promising agents. The hope is that introducing these earlier could prolong endocrine therapy duration and prevent emergence of resistant clones. |
Dr. Gary Grad: As one of the investigators on SERENA-6, are there any final thoughts you’d like to share about the paradigm shift we’re seeing with SERENA and PADA-1, and where things are headed from your perspective? |
| Dr. Cynthia Ma: Yes. I think SERENA-6 really is paradigm-shifting. As you mentioned earlier, it also raises the broader question of whether we might eventually intervene earlier for other targetable mutations as they emerge. That’s an area that will require prospective studies, but it’s an important direction for the field. Dr. Gary Grad: One key point you raised that I think deserves emphasis is the quality-of-life data from SERENA-6. It showed not only improved PFS and delayed time to next treatment, but also delayed quality-of-life deterioration and even improvement in some cases… |
Outro
Tempus’ xF+ assay offers highly sensitive, broad-panel ctDNA monitoring to detect emerging ESR1 mutations, providing clinicians with actionable insights for timely therapy decisions. By enabling earlier intervention, these tools have the potential to improve patient outcomes, prolong endocrine therapy effectiveness, and support quality-of-life preservation—helping bring the promise of precision oncology into routine clinical care. Learn more about how Tempus xF and xF+ can support monitoring for ESR1 alterations here. |
-
 03/04/2026
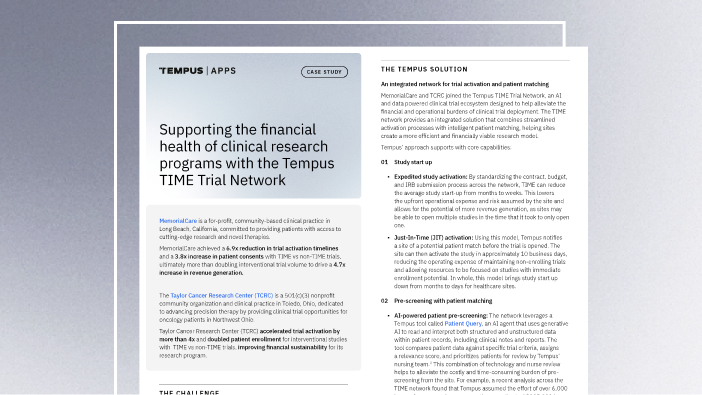
03/04/2026Supporting the financial health of clinical research programs with the Tempus TIME Trial Network
By combining the power of AI-driven technology with a streamlined operational model, Tempus provides the infrastructure and support to enable sites with limited resources to participate in research and expand their capabilities.
Read more -
 01/20/2026
01/20/2026From image to insight: How Tempus is leveraging AI to advance biomarker screening at scale
By leveraging Paige Predict to screen for genomic and phenotypic biomarkers, clinicians and researchers have rapid access to valuable information to prioritize testing and pre-screen patients at scale.
Read more -
 12/04/2025
12/04/2025Pioneering decentralized oncology trials: Success at the nation’s largest community practices
Hear directly from industry leaders and pioneering site partners as they share insights on expanding their research footprint and improving financial sustainability for their institutions.
Watch replay