-
PROVIDERS
Learn more
Join Tempus at the 2026 ASCO® Annual Meeting!
-
LIFE SCIENCES
REGISTER NOW
From insight to impact: Leveraging the AI-enabled Next platform with BMS to advance equitable access in precision oncology
-
PATIENTS
It's About Time
View the Tempus vision.
- RESOURCES
-
ABOUT US
View Job Postings
We’re looking for people who can change the world.
- INVESTORS
03/22/2024
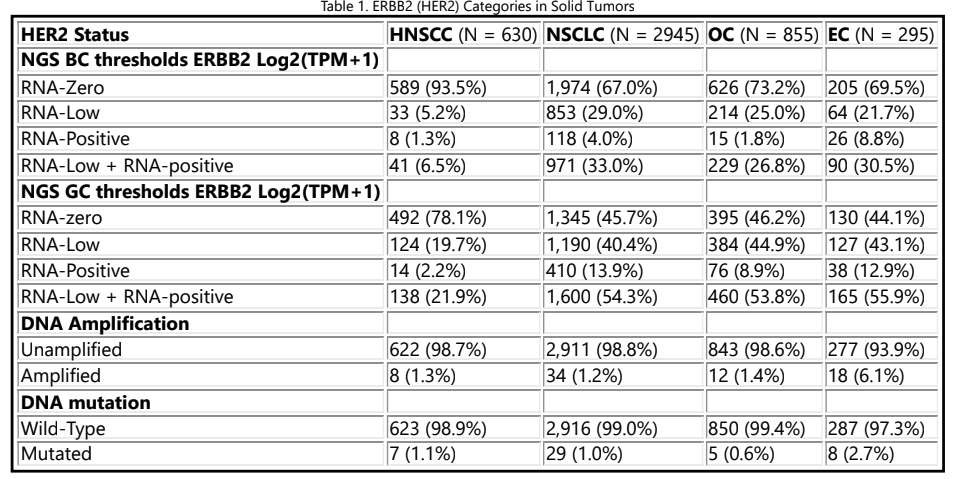
Analysis of HER2 Prevalence by RNA Expression Across Solid Tumors
AACR 2024
PRESENTATION
Authors
Katherine Moxley, Emilie Scherrer, Martin Bontrager, Samantha Whitman, Naomi R. M. Schwartz, Chithra Sangli, Seung Won Hyun, Halla Nimeiri, Jonathan Ball, Charu Aggarwal
Background: The frequency of HER2 expression in solid tumors other than breast (BC) and gastric cancer (GC) is not well defined. This study describes the frequency of HER2 expression by correlating HER2 IHC/ ISH and ERBB2 mRNA levels by NGS in tumor samples of patients with locally advanced/metastatic (LA/m) BC or GC and applying those findings to predict HER2 expression in other solid tumors.
Methods: De-identified records from NGS-tested patients with LA/m BC, GC, HNSCC, NSCLC, endometrial, and ovarian cancers in the Tempus database from 2015 – 2021 were analyzed. Patients with BC and GC who underwent HER2 IHC/ISH testing were categorized as: RNA-zero (IHC0), -low (IHC1+, IHC2+/ISH-), and -positive (HER2+; IHC2+/ISH+, IHC3+). To identify thresholds separating HER2 subgroups, a logistic regression model was fit to NGS and IHC status data in BC and GC. These thresholds were applied to other solid tumors to predict the distribution of HER2 expression. HER2 amplification and mutation rates were evaluated in the Tempus NGS data.
Results: Logistic regression modeling used 3,898 samples. HER2+ samples had the highest IHC-to-RNA agreement at 80% (BC) and 81% (GC) compared to HER2 low and zero samples which ranged ~56-75% agreement. When applying thresholds identifying RNA-low and RNA-positive sample to other tumors (N = 4,726), the models predicted up to 33% (BC thresholds) or 56% (GC thresholds) of tumors express HER2 at levels that may be detectable (Table 1).
Conclusions: A notable amount of solid tumors apart from BC or GC have RNA expression that may correspond to HER2 IHC ≥1+. This opens the possibility for novel agents such as HER2-directed antibody drug conjugates to impact patient care in several tumor types. Further IHC testing in these populations are needed to corroborate our results.